
Projecting the Future of the AIDS Epidemic
In a companion blog, I pointed out that the long-term effect of President Trump’s proposed cuts in PEPFAR funding will be much larger than the estimated one million lives discussed in a recent New York Times article. If the 20% cut is permanent, and other countries follow the American lead, then up to 16 million people may needlessly die of AIDS-related causes by the year 2030.
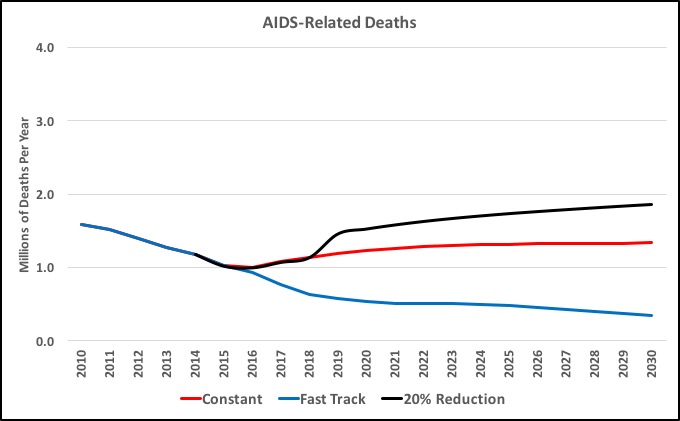
Predicting the future is always uncertain, especially when dealing with the medical, social, economic, and political complexities of the AIDS epidemic. So let me explain where the numbers came from. The starting point for my analysis was a report issued by UNAIDS in April 2016. The 2016 report was an updated version of a December 2014 report that had been based on a collaborative study with The Lancet medical journal. Both the original report and the 2016 update included projections about the AIDS epidemic through 2030 under two different scenarios of global investment in the AIDS response. In one scenario, the world collectively invests the same amount per year that we are already investing, about $19.2 billion. The rate of AIDS-related deaths rises gradually to about 1.3 million per year in 2030. In the other scenario, the world increases its investment to about $26.2 billion per year in 2020 with a slight reduction after that. The rate of deaths declines to about 400,000 per year. In this second scenario, the number of new infections also declines substantially, effectively ending HIV/AIDS as a public health threat by 2030. These two scenarios are the red and blue lines in the chart.
The black line shows a third scenario, namely, a reduction of 20% in the overall global response to the AIDS epidemic. Under this scenario, the number of deaths rises significantly to about 1.9 million per year. The projections for the third scenario reflect some modeling I have done to understand the consequences of a reduction in the global response to the AIDS epidemic. My model is based on the UNAIDS model, with two additional effects. First, if the global response is reduced, then the global supply of ARVs (anti-retroviral medicines) would be reduced. Many people who are currently receiving medication would no longer receive it. In this case, the number of people on treatment is reduced by 20% in 2018. The number of deaths is a function of the number of people living with HIV who are not on treatment, so in this case, the number of deaths goes up significantly in 2019, then rises more gradually. The second effect of a drop in the global response would be a weakening of prevention and testing initiatives, either in scope or in effectiveness. Generally, new infections are a function of the number of people living with HIV who are not on treatment and who have not reached viral suppression, combined with the effectiveness of prevention initiatives. In this case, the prevention effectiveness factor went down by 20% in 2018. The combined result of these two effects is the black line in the chart.
When the reports by UNAIDS and The Lancet were released in 2014, no one seriously worried about a significant drop in the global response to the AIDS epidemic. I remember discussions last year with other AIDS activists at the United Nations High-Level Meeting on AIDS in New York and at the International AIDS Conference in Durban. We thought the challenge would be to ensure that the world increased its investment in order to fully implement the Fast Track strategy. We feared we might not get the full commitment, but we assumed things would at least go along at the current level. It is frightening to realize that we must now consider much worse scenarios..
Note: If you know of other attempts to model the effects of reducing the global response to AIDS, or you are interested in more details about the model I used, please contact me at davidb@waragainstaids.org.